


Background
Nepal is one of the world’s least developed countries where problems related to transportation, lack of education, lack of proper healthcare services and cultural beliefs restrict access to healthcare services for many.
Although the government of Nepal has been working to provide better healthcare services, Nepal is still among the countries with the highest maternal and neonatal mortality rates in the world.
Postnatal care (PNC) is a critical period of maternal care, as serious and life threatening complications for mother and newborn can occur in this period. Despite this, less than 20% of new mothers in Nepal attend the three postnatal checkups recommended to be carried out within the first week after delivery.
Outcomes and objectives
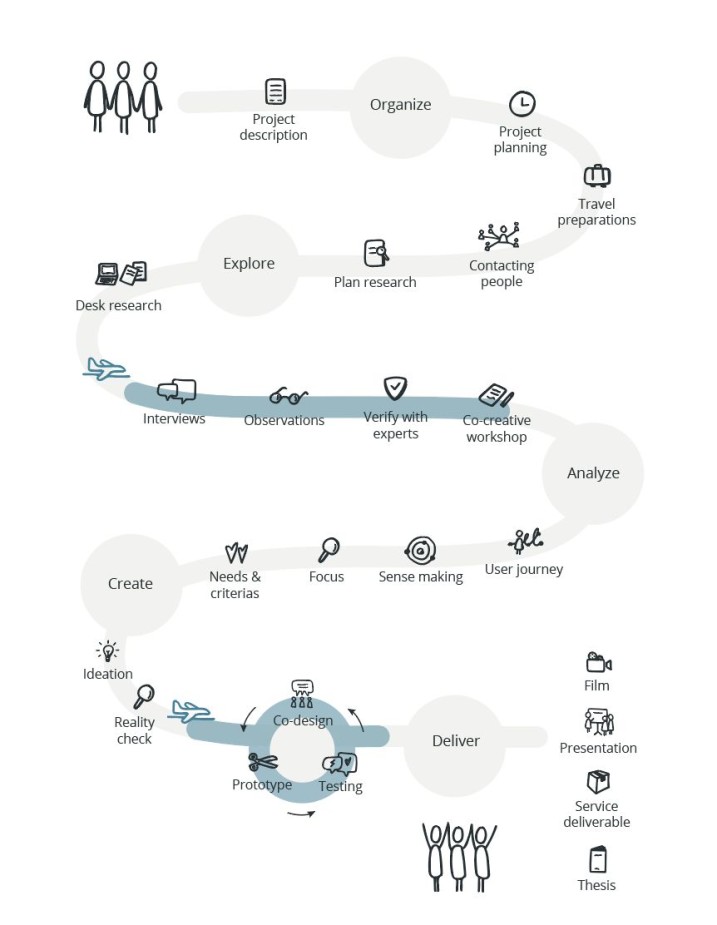
The aim of the master thesis was to put service design methodology for the developing world into practice.
We intended to carry out a design project from inspiration to implementation that met the needs of users in their own cultural and geographical circumstances. The project goal developed into raising awareness and knowledge about the importance of PNC in an effort to increase the PNC checkup rate in rural areas of Nepal.
It was found that a lack of autonomy, education, access to services, economic issues and strong cultural traditions prevented women, specifically in rural areas, from utilizing healthcare services during the postnatal period.
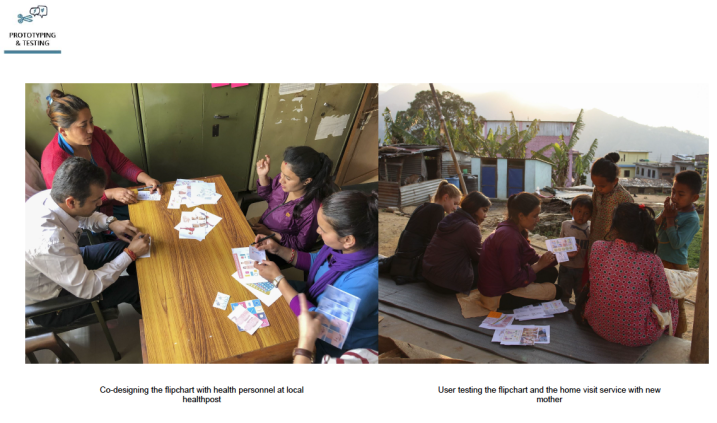
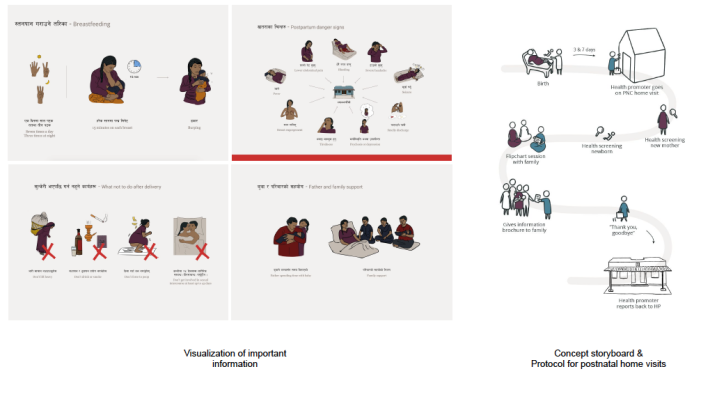
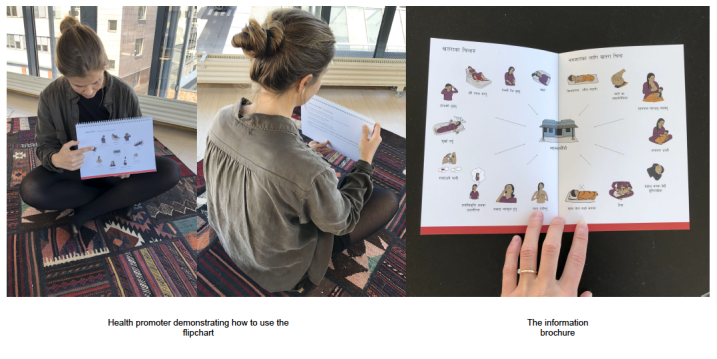
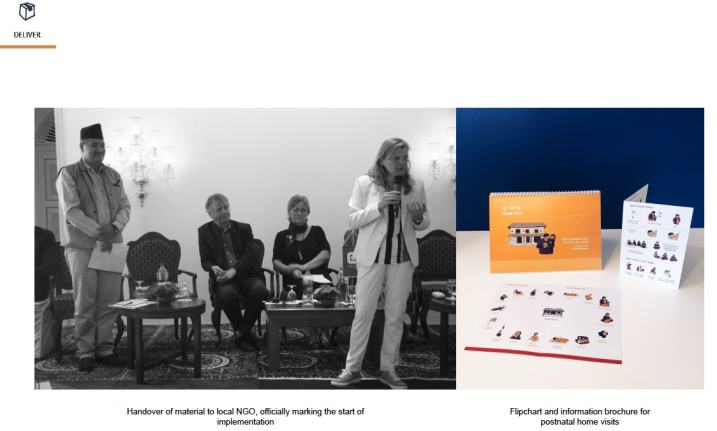
The project resulted in highlighting the importance of proper postnatal healthcare by co-creating and designing a new health service for postnatal home visits for women who are not able to access a health facility for postnatal checkups. The service includes a protocol for the visits, as well as a flipchart and brochure with visualizations of important information for the postnatal period, with the intention of educating the new mother and her family.
Target market
New mothers in rural areas of Nepal and their families.



Share your thoughts
0 RepliesPlease login to comment