Output
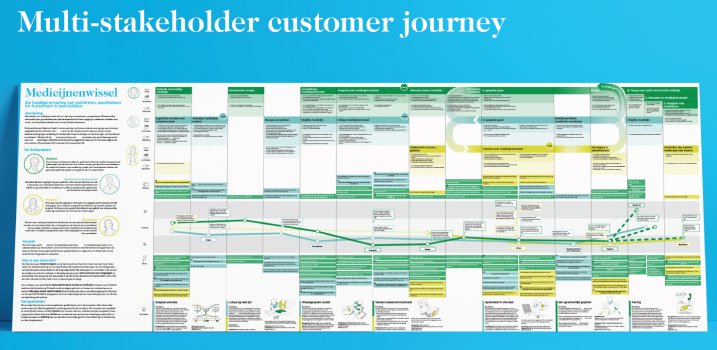
The insights from the explorative interviews were used to create a customer journey.¹ This is a multiple stakeholder customer journey, which allows you to see the connections in the journey among all relevant stakeholders. This customer journey has been used as a tool for innovation, but is also used as a way to convey the problems at hand and to present the seriousness of the matter.
The visualisation is used by team members to look back on when working on the subject, but also to create support in the organisations of all stakeholders. On the left-hand side of the visualisation, you see a short introduction of the subject, followed by the target groups of the project. Then, a short explanation of our approach is given, after which we explain how to interpret a customer journey. Finally, there is a description of several areas of opportunity that we have found in the journey, where we feel it is most important to improve the current situation.
For each target group, we have three ‘swimming lanes’: the name of the phase, the activities that the target user can perform during this phase and the needs that are present in that phase. The next element in the customer journey - which really carries the meaning of the journey and conveys how the target groups feel - is the experience curve. You see that there are 3 lines in the experience curve, one for each target group. Note that the GP and specialist are combined, since their phases in the journey are the same.
The experience curve is enriched with quotes from the interviews, as well as descriptions of the emotions that the target groups are experiencing. Above the experience curve, you can find the gains that are experienced by the target groups, each depicted by their own color. Below the experience curve you can find the pains that they experience. At the bottom of the customer journey, the 7 concepts nominated for further development are visualised with a brief description. These are the concepts that resulted from the co-creative ideation session. One of the most interesting takeaways from the customer journey is the ‘loop’ that patients tend to find themselves in when looking for answers. They contact various parties (mostly GP, pharmacy and healthcare insurer) but are “sent from pillar to post”.
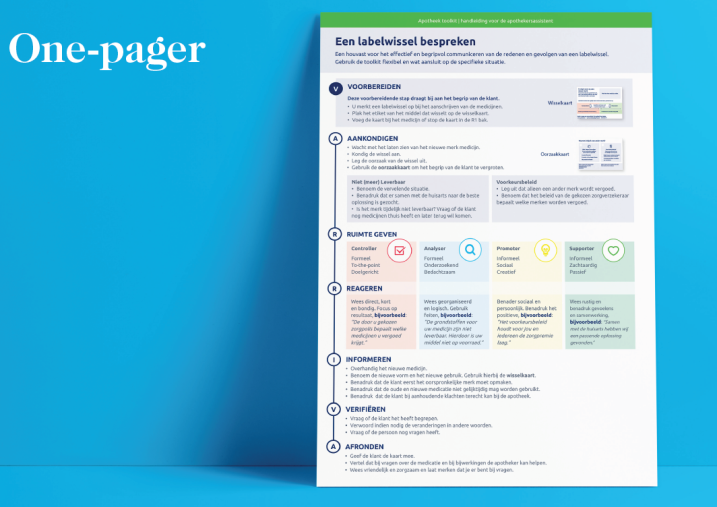
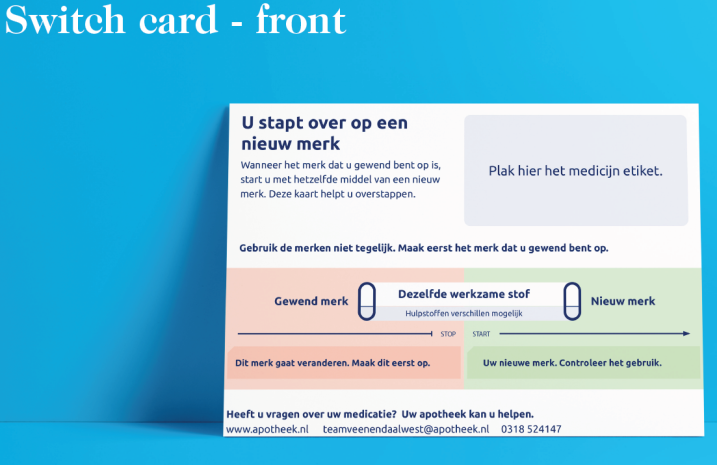
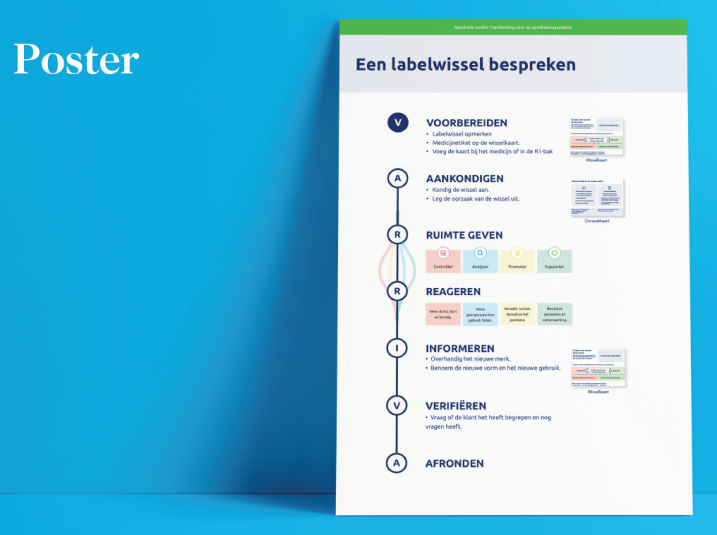
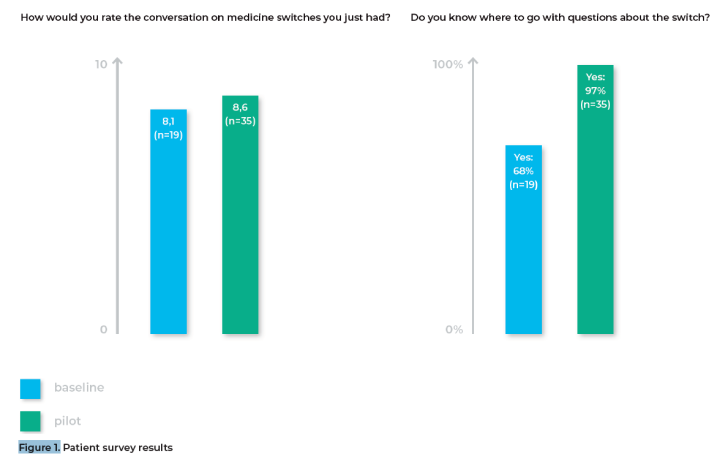
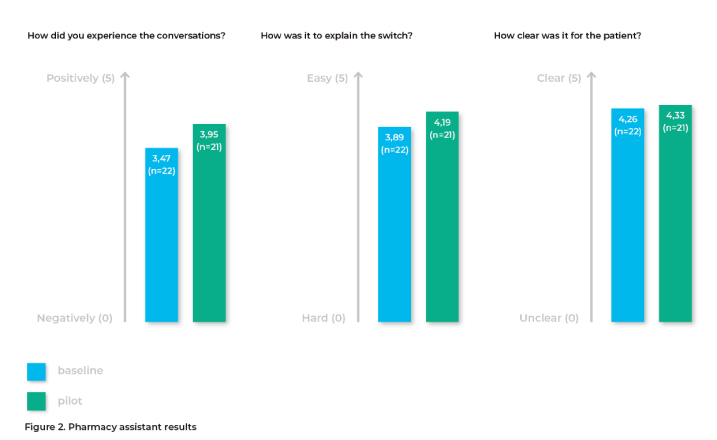
As stated in the introduction, the first result of the project is a toolkit for pharmacists that describes the best way to carry out the conversation at the counter: the first time it becomes clear for a patient that a medicine switch has occurred for him/her. It also includes visual aids for the patient, that help him/her to understand the complex and confusing situation. This result has been created through different rounds of iterations: after internal discussions, two separate focus groups and two separate pilots.
The surveys used during the pilots - for both the pharmacy assistants and the patients - have been added to the visual document. During the pilot, the assistants were instructed on how to use the toolkit and the visual aids. A scenario to help with this instruction is added to the visual document. It is important to note that in every pharmacy the way of working can be slightly different. This required flexibility in how to use the toolkit during the pilot and will require the same flexibility to find a way of working that works for the specific pharmacy it’s launching in.







Share your thoughts
0 RepliesPlease login to comment